India National Strategic Plan (NSP) for TB 2017 - 2025
The Indian TB National Strategic Plan (NSP) 2017 - 2025 was the plan produced by the government of India (GoI) which set out what the government believed was needed to eliminate TB in India. The NSP 2017 - 2025 described the activities and interventions that the GoI believed would bring about significant change in the incidence, prevalence and mortality from TB. This was in addition to what was already going on in the country.
The NSP set out the recommendations of the GoI. However, the rate at which these recommendations were to be implemented, would largely depend on the action taken by individual states. The state of Uttar Pradesh had the highest number of TB patients notified by both the public and private sector.
By 2020 it was clear that the National Strategic Plan (NSP) was not on course to achieve the elimination of TB by 2025. So a new NSP was developed, the NSP India 2025 which replaced the NSP 2017 - 25.
In addition, this new NSP identified a significant number of major initiatives which still needed to be carried out by the NTEP.
Visions & Goals of the National Strategic Plan 2017 - 2025

TB multimedia campaign in India, INDIAVsTB encourages people to get tested for TB, an important part of the NSP.
The Vision is of a TB free India with zero deaths, disease and poverty due to tuberculosis
The Goal was to achieve a rapid decline in the burden of TB, mortality and morbidity, while working towards the elimination of TB in India by 2025.
The requirements for moving towards TB elimination in India were arranged in four strategic areas of
Detect, Treat, Prevent & Build.There is also across all four areas, an overarching theme of the Private Sector. Another overarching theme is that of Key Populations.
Targets
The targets of the National Strategic Plan were set out as consisting of both outcome and impact indicators. There were also four main “thrust” or priority areas in the NSP which were:
- Private sector engagement;
- Plugging the “leak” from the TB care cascade (i.e. people with TB going missing from care);
- Active case finding among key populations;
- and for people in “high risk” groups, preventing the development of active TB in people with latent TB.
Another “thrust” area was that of the Programmatic Management of Drug Resistant TB (PMDT).
Detect
The aim is to detect all those people with drug sensitive TB as well as those with drug resistant TB. The emphasis is to be on reaching TB patients seeking care from private providers and also finding people with undiagnosed TB in “high risk” or key populations. This was to be done through:
- Scaling up free, high sensitivity TB diagnostic tests such as CBNAAT;
- Scaling up private provider engagement approaches;
- Universal testing for drug resistant TB;
- & Systematic screening of high risk populations.
Diagnosis
The Technical & Operational Guidelines for TB Control (TOG) described how various tests should be used to diagnose anyone who has signs and symptoms suggesting that they might have TB. The tests to be used were sputum smear microscopy, chest X ray and the CB-NAAT test. The CB-NAAT test was beginning to be made available throughout India. There is a diagram, or set of rules, which shows which tests should be used for different groups of people.
There is a further explanation on the page on Testing & diagnosis of TB in India.
Active case finding
The main objective of active case finding (ACF) is to detect TB cases early and to initiate treatment promptly. The NSP emphasizes the need to shift from passive case finding, which is waiting for people to seek care, to ACF which involves seeking out people in targeted groups.
In Karnataka 1,150 cases of TB were identified in just the first week of active case finding.1
Treat
Initiate and sustain all patients on appropriate anti-tb treatment wherever they seek care. Provide patient friendly systems and social support. This wasto be done through:
- Preventing the loss of TB cases in the cascade of care by providing support systems. The “cascade of care” means every step in the provision of treatment, from when it is first started, to the point at which the patient finishes their treatment and is cured of TB;
- Providing free TB drugs for all patients with TB;
- Provide daily TB drugs for all patients with TB and a rapid scale up of short course regimens for drug resistant TB. Provide treatment approaches guided by drug sensitivity testing.
- Providing patient friendly adherence monitoring and social support in order to sustain TB treatment;
- & The elimination of catastrophic costs by linking eligible TB patients with social welfare schemes including providing nutritional support.
TB drugs were free at government centres. The NSP plan was that eventually TB drugs would be available free from private centre pharmacies as well. Currently it was believed that only half of all TB patients made use of the free medicines. It is believed that making the TB drugs available in private hospitals:
"will also help remove the stigma among that section of society which is hesitant to approach government run centres for taking medicines"Jagdish Prasad, Director General of Health Services
Nutritional support for patients with TB
It was then announced that patients with TB would receive R500 ($8) a month for food. There is more about all the Direct Benefit Transfer schemes for TB.
Under nutrition is a risk factor for TB in India. Under nutrition worsens the nutritional status, generating a vicious cycle which can lead to adverse outcomes during and after treatment for patients with active TB. This includes those with MDR-TB. So this payment was partially to ensure that patients with TB have adequate food. There is more about food and TB and nutrition & TB.
Prevent
Preventing the emergence of TB in susceptible populations. This was to be done through
- Scaling up air-borne infection control measures at health care facilities;
- Providing treatment for latent TB infection for the contacts of people with confirmed TB;
- & Addressing the social determinants of TB through an approach across different sectors. The social determinants of health are generally considered to be the conditions in which people live and work that affect their health.
Build
Build and strengthen relevant policies. Provide extra capacity for institutions and extra human resources capacity. This is to be done through:
- Translating high level political commitment into action;
- Restructuring the RNTCP, now known as the NTEP and other institutional arrangements;
- Building supportive structures for surveillance, research and innovations. Providing a range of interventions based on the local situation;
- Scaling up technical assistance at national and state levels;
- & Preventing the duplication of partners’ activities
Private Sector
Private provider engagement
 At least half of those treated for TB in India first attend the largely unorganized and unregulated private sector. Patients from low income households will often lose several months of their income in the process of paying for inappropriate diagnostics and treatments before starting approved therapy.
At least half of those treated for TB in India first attend the largely unorganized and unregulated private sector. Patients from low income households will often lose several months of their income in the process of paying for inappropriate diagnostics and treatments before starting approved therapy.
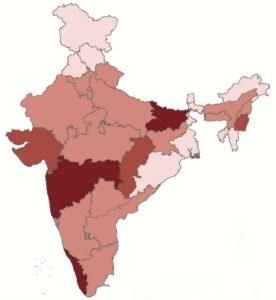
Statewise proportion of notification of patients from private sector in 2016
Patients treated by private providers have often not been notified to the NTEP, despite government orders to that effect. Patients cared for by private providers rarely receive sputum testing, and DST. Similarly, public health services such as surveillance, adherence monitoring, contact investigation, and outcome recording rarely reach privately treated patients.
A recent study of private doctors showed that only 29% of doctors had adequate knowledge of diagnosis, and only 29% knew a proper treatment regimen.2
There was now to be a major change in the way that the NTEP engaged with private providers. Partnership was to be the way forward. The previous approach was for private providers to direct people to the RNTCP to receive their care in the public sector. Now the approach was to be for the public sector NTEP to work with the private sector, assisting the private sector to provide high quality care.
The new strategy for reaching patients in the private sector amounted to a total change in the way that the RNTCP engaged with private providers. The new strategy was going to be systematic and large scale, rather than ad hoc and insignificant. Rather than the public sector competing with private providers the NTEP would work with them to deliver quality TB services to the entire population.
The aim was for the annual number of TB cases notified by private providers to increase ten fold, from 0.2 to 2 million annually. That is private providers should be providing 56% of total case notifications by 2020. For the first time there would also be a budget appropriate to both the size of the problem and the opportunity of private sector care.
The approach would be to firstly capture all TB patients by attracting notification from private providers and then work to improve the quality of care. Private providers would be provided with incentives. There is more about all the Direct Benefit Transfer schemes for TB.
Key Populations
Key populations are generally regarded as people who are socially vulnerable and people who are clinically high risk. They face barriers in accessing care. ACF in vulnerable groups was to be a focus of the NSP over the next five years. Some of the priority groups are as follows:
Vulnerable Groups for NSP 2017 - 2025
| Priority | Urban area | Rural area | Tribal area |
|---|---|---|---|
| 1 | Slum | Difficult to reach villages | Difficult to reach villages and hamlets |
| 2 | Prison inmates | Mine workers | Villages with known higher case load |
| 3 | Old age homes | Stone crusher workers | Tribal school hostels |
| 4 | Construction site workers | Population groups with known high malnutrition | Area with known high malnutrition |
| 5 | Refugee camps | Populations known to drink raw milk | Villages seeking care from traditional healers |
| 6 | Night shelters | Populations known to eat uncooked meat | Populations known to drink raw milk |
The Cost of the NSP 2017 - 2025
The cost of the NSP was going to depend on the pace of implementation of the strategy, the demand from states, and the availability of resources. It was expected that the cost of implementing the new NSP would be Rs 16,649 (USD 2,485 million). This would be a significant increase over the budget for the NSP 2012-2017.
How was the progress of the India TB NSP to be monitored
A national level annual review of the NSP would be undertaken.
There are some main NSP impact indicators, some main outcome indicators as well as some results indicators for PMDT.
What progress was made in the first three years from 2017 - 2019?
The outcome indicator for TB patient notifications for 2020 was that 3,600,000 notifications should be made. The indicator for private providers was that 2 million notifications should be made.
So looking at these and other indicators, it seemed unlikely that the goal of elimination by 2025 would be reached.
So this NSP was replaced by a new NSP the NSP 2020 - 2025.
Outcome Indicators for NSP 2017 - 2025
| Priority | 2020 | 2023 | 2025 | |
|---|---|---|---|---|
| 1 | Total TB patient notifications | 3.6 mil | 2.7 mil | 2 mil |
| 2 | Total patient notifications from private providers | 2 mil | 1.5 mil | 1.2 mil |
| 3 | No. of MDR/RR patients notified | 92,000 | 69,000 | 55,000 |
| 4 | Proportion of notified patients offered DST | 80% | 98% | 100% |
| 5 | Proportion of notified patients initiated on treatment | 95% | 95% | 95% |
| 6 | Treatment success rate among notified DSTB | 90% | 92% | 92% |
| 7 | Treatment success rate among notified DRTB | 65% | 73% | 75% |
| 8 | Proportion of identified targeted key affected population undergoing active case finding | 100% | 100% | 100% |
| 9 | Proportion of notified TB patients receiving financial support through DBT | 80% | 90% | 90% |
Results Indicators for NSP 2017 - 2025
| Results Indicator | 2017 | 2018 | 2020 | 2025 |
|---|---|---|---|---|
| Proportion of notified patients offered DST | 50% | 60% | 80% | 100% |
| No. of presumptive DRTB patients to be examined | 600,000 | 700,000 | 1,100,000 | 1,500,000 |
| No. of MDR/RR patients notified | 53,460 | 66,000 | 92,000 | 55,000 |
| No. of MDR/RR patients initiated on treatment | 48,114 | 59,400 | 82,800 | 49,500 |
| No. of XDR TB patients notified | 2,406 | 2,970 | 4,140 | 2,475 |
| No. of XDR TB patients initiated on treatment | 2,165 | 2,673 | 3,726 | 2,228 |
| Treatment success rate for MDR/RR TB | 48% | 48% | 65% | 75% |
Impact Indicators for the National Strategic Plan 2017 - 2025
| Impact Indicator | 2020 | 2023 | 2025 |
|---|---|---|---|
| To reduce estimated TB incidence (rate per 100,000) | 142 | 77 | 77 |
| To reduce estimated TB prevalence (rate per 100,000) | 170 | 90 | 65 |
| To reduce estimated mortality due to TB (per 100,000) | 15 | 6 | 3 |
| To achieve zero catastrophic costs for affected families due to TB | 0% | 0% | 0% |
Page Updating
This page was last updated in April 2022.
Author Annabel Kanabus
Social Media & Web Site Linking
If you have found this page useful please tell other people about TBFacts and if you have a website please link to us at https://tbfacts.org/tb-india-nsp/.
Footnotes
- Reshma Ravishanker, "1,150 TB cases detected in a week in Karnataka", 2019, https://www.deccanherald.com/state/1150-tb-cases-detected-in-a-week-in-karnataka-750061.html[↩]
- “To eradicate TB, many doctors must first learn how to diagnose it”, 2018, New Indian Express, http://www.newindianexpress.com/thesundaystandard/2018/feb/03/to-eradicate-tb-many-doctors-must-first-learn-how-to-diagnose-it-1767881.html[↩]
Would you like to send us a comment about this page?