What tests are there for TB?
There are tests which can diagnose TB. There are also tests to find out if someone has TB bacteria that are susceptible to TB drug treatment. If the bacteria are susceptible to treatment, it means that the treatment should work. The opposite of being susceptible to treatment is being drug resistant. A TB test to find out if someone has drug resistant TB, is known as a drug susceptibility test.
Even if a person has symptoms of TB it is often difficult to diagnose TB, and it is particularly difficult to diagnose rapidly. Rapid diagnosis is what is needed to provide effective TB treatment.
The accuracy of tests
Some of the current tests take a long time to obtain a result, and some are not very accurate. They either have low sensitivity (the ability to correctly detect people with TB) and/or low specificity (the ability to correctly detect people who haven’t got TB).
If a test has low sensitivity, it means that there will be a significant number of “false negatives”. This means that the result suggests that a person has not got TB when they actually have got it. Similarly, a low specificity means that there will be a significant number of “false positives” suggesting that a person has TB when they actually haven’t.
The most accurate tests such as culture take a long time to do. Some tests are also very expensive and require complex laboratory facilities.
Culture Test
Although the culture test for TB is very accurate, it can take several weeks to get a result. It also requires expensive equipment and skilled personnel.
The skin test
The skin test is widely for diagnosing TB. In countries with low rates of TB it is often used to test for latent TB infection. The problem with using it in countries with high rates of TB infection is that the majority of people may have latent TB.
The skin test involves injecting a small amount of fluid (called tuberculin) into the skin in the lower part of the arm. Then the person must return after 48 to 72 hours to have a trained health care worker look at their arm. The health care worker will look for a raised hard area or swelling, and if there is one then they will measure its size. They will not include any general area of redness.1

A health care worker measures the size of the reaction to the tuberculin skin test © CDC
The test result depends on the size of the raised hard area or swelling. The larger the size of the affected area the greater the likelihood that the person has been infected with TB bacteria at some time in the past. But interpreting the skin test result, that is whether it is a positive result, may also involve considering the lifestyle factors of the person being tested for TB.2 The skin test also cannot tell if the person has latent TB or active TB disease.
The Mantoux TB is the type of test most often used, although the Heaf and Tine tests are still used in some countries. None of these tests though will guarantee a correct result. False positive results happen with the skin test because the person has been infected with a different type of bacteria, rather than the one that causes TB. It can also happen because the person has been vaccinated with the BCG vaccine. This vaccine is widely used in countries with high rates of TB infection. False negative results particularly happen with children, older people and people with HIV.
TB Interferon gamma release assays (IGRAs)
The Interferon Gamma Release Assays (IGRAs) are a new type of more accurate test. In this context referring to an assay is simply a way of referring to a test or procedure.

T-SPOT® Test for TB © Oxford Immunotec
IGRAs are blood tests that measure a person’s immune response to the bacteria that cause TB. The immune system produces some special molecules called cytokines. These TB tests work by detecting a cytokine called the interferon gamma cytokine. In practice you carry out one of these TB tests by taking a blood sample and mixing it with special substances to identify if the cytokine is present.
Two IGRAs that have been approved by the U.S. Food and Drug Administration (FDA), and are commercially available in the U.S., are the QuantiFERON® TB Gold test, and the T-SPOT® TB test.
The advantages of an IGRA includes the fact that it only requires a single patient visit to carry out the TB test. Results can be available within 24 hours, and prior BCG vaccination does not cause a false positive result. Disadvantages include the fact that the blood sample must be processed fairly quickly, laboratory facilities are required, and the test is only for latent TB. It is also thought that the IGRAs may not be as accurate in people who have HIV.3 In low prevalence resource rich settings, IGRAs are beginning to be used in place of the TB skin test.4
Sputum smear microscopy as a test for TB
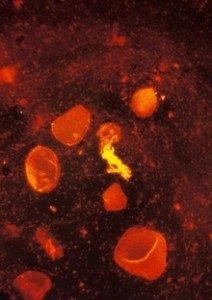
A test for TB, a sputum smear stained using fluorescent acid fast stain © CDC/R W Smithwick
Smear microscopy of sputum is often the first test to be used in countries with a high rate of TB infection. Sputum is a thick fluid that is produced in the lungs and the airways leading to the lungs. A sample of sputum is usually collected by the person coughing. Several samples of sputum will normally be collected.5 In 2012 it was suggested that two specimens can be collected on the same day without any loss of accuracy.6 7
To do the test a very thin layer of the sample is placed on a glass slide, and this is called a smear. A series of special stains are then applied to the sample, and the stained slide is examined under a microscope for signs of the TB bacteria.8
Sputum smear microscopy is inexpensive and simple, and people can be trained to do it relatively quickly and easily. In addition the results are available within hours. The sensitivity though is only about 50-60%.9 In countries with a high prevalence of both pulmonary TB and HIV infection, the detection rate can be even lower, as many people with HIV and TB co-infection have very low levels of TB bacteria in their sputum, and are therefore recorded as sputum negative.
In some countries sputum smear microscopy is being phased out, and is being replaced by molecular tests.
Fluorescent microscopy
The use of fluorescent microscopy is a way of making sputum tests more accurate. With a fluorescent microscope the smear is illuminated with a quartz halogen or high pressure mercury vapour lamp, allowing a much larger area of the smear to be seen and resulting in more rapid examination of the specimen.
One disadvantage though is that a mercury vapour lamp is expensive and lasts a very short time. Such lamps also take a while to warm up, they burn significant amounts of electricity, and electricity supply problems can significantly shorten their life span. One way of overcoming these problems is the use of light emitting diodes (LEDs). These switch on extremely quickly, have an extremely long life, and they don’t explode.10
In 2011 the World Health Organisation issued a policy statement recommending that conventional fluorescence microscopy should be replaced by LED microscopy. It also recommended that in a phased way, that LED microscopy should replace conventional Ziehl-Neelsen light microscopy.11z

A man receives a chest X-Ray during the admission process at a hospital in India. © David Rochkind
Chest X-ray
If a person has had TB bacteria which have caused inflammation in the lungs, an abnormal shadow may be visible on a chest x-ray.12 Also, acute pulmonary TB can be easily seen on an X-ray. However, what it shows is not specific. A normal chest X-ray cannot exclude extra pulmonary TB.
Also, in countries where resources are more limited, there is often a lack of X-ray facilities.
Serological tests as a test for TB
Serological tests are carried out on samples of blood, and they claim to be able to diagnose TB by detecting antibodies in the blood. However, testing for TB by looking for antibodies in the blood is very difficult.
As a result serological TB tests, sometimes called serodiagnostic tests, are inaccurate and unreliable. The World Health Organisation has warned that these tests should not be used to try and diagnose active TB. Some countries have banned the use of serological or serodiagnostic tests for TB.
Serological tests for TB are very different from the IGRA tests described above.
Molecular tests
Some new molecular tests such as the Genexpert test and the TrueNat test are now available. The TrueNat was approved by the World Health Organisation (WHO) in 2020. The WHO has produced guidelines on the use of different tests.
Tests for TB summary
There is no single test that can be used to test for TB in all circumstances. Some tests are cheap but not very accurate. Some can only be used to test for TB and cannot test for drug resistance. Others such as the TB culture test, the new Genexpert and the TrueNat group of tests can be used to diagnose TB and they can also test for some types of TB drug resistance.
With the development of the new molecular tests there is beginning to be significant progress. Although there are some issues about the speed with which patients are provided with treatment after receiving a diagnosis, faster diagnosis must surely be a key factor in controlling the TB epidemic in resource poor countries.
Page Updating
This page was last updated in June 2022.
Author Annabel Kanabus
Social Media & Web Site Linking
If you have found this page useful please tell other people about TBFacts.org, and if you have a web site please link to us at https://tbfacts.org/tests-tb/.
Footnotes
- “TB Testing & Diagnosis”, CDC www.cdc.gov/tb/topic/testing/[↩]
- “http://www.cigna.com/individualandfamilies/health-and-well-being/hw/medical-tests/tuberculin-skin-test-hw203560.html”, Cigna
http://www.cigna.com/individualandfamilies/health-and-well-being/hw/medical-tests/[↩] - “Guidelines for intensified case finding and isoniazid preventative therapy for people living with HIV in resource constrained settings”, Geneva, WHO, 2011 9
http:/www.who.int/tb/publications/2011/[↩] - “Fact Sheets Interferon-Gamma Release Assays -Blood Tests for TB Infection”, CDC www.cdc.gov/tb/publicationsfactsheets/[↩]
- “Sputum Culture”, WebMD www.webmd.com/lung/sputum-culture[↩]
- Davis, J Lucian “Diagnostic accuracy of same-day microscopy versus standard microscopy for pulmonary tuberculosis: a systematic review and meta-analysis”, The Lancet Infectious Diseases 23rd October 2012 www.thelancet.com/[↩]
- Kirwan, Daniela E “Same-day diagnosis and treatment of tuberculosis”, The Lancet Infectious Diseases 23rd October 2012
www.thelancet.com/[↩] - “Sputum Gram stain - Overview”, University of Maryland Medical Center
www.umm.edu/ency/article/[↩] - Siddiqi, Kamran “Clinical diagnosis of smear-negative pulmonary tuberculosis in low-income countries: the current evidence”, The Lancet Infectious Diseases, Vol 3, May 2003, 288
www.thelancet.com/journals/[↩] - “TB diagnosis: Improving the yield with fluorescence microscopy”, 2007
www.aidsmap.com/TB-diagnosis-Improving-the-yield-with-fluorescence-microscopy/[↩] - “Fluorescent light-emitting diode (LED) microscopy for diagnosis of tuberculosis”, WHO, 2011
www.who.int/tb/areas-of-work/laboratory/policy_statements/en/[↩] - “Tuberculosis (TB): Diagnosis”, National Jewish Health
www.nationaljewish.org/healthinfo/Conditions/tb/diagnosis[↩]
Would you like to send us a comment about this page?